
The Unaddressed Opportunity in Indian Reproductive Medicine
In my years consulting for fertility practices across the subcontinent, I have noticed a persistent, almost cultural blind spot in the evolving landscape of Indian reproductive medicine. Historically, our gaze has been fixed firmly on female factor infertility. We investigate the uterus, the ovaries, and the tubes with relentless precision. Yet, recent epidemiological data forces us to confront a hard truth: we are missing half the picture.
Today, male factor issues are the primary driver in nearly 40% to 50% of all conception failures. For the modern Gynecologist and the aspiring clinic owner, developing a granular understanding of Male Infertility Causes is no longer just an exercise in diagnostic diligence—it is the absolute cornerstone of establishing a successful, comprehensive, and frankly, profitable IUI clinic.
I’ve seen it happen time and again in OPDs from Mumbai to Tier-2 towns. A couple walks in. The focus immediately shifts to the wife. Meanwhile, the male partner—who may be suffering from severe oligospermia or high DNA fragmentation—is sidelined until multiple cycles fail. Despite the high prevalence of these male factor issues, a shocking number of gynecological practices in India lack the specialized Andrology infrastructure to manage these cases in-house.
The result? A fragmented patient journey. You refer the couple out to a urologist or a corporate IVF chain. In doing so, you lose control of the treatment cycle. And, let’s be honest about the business side of medicine: you are handing over significant revenue to another facility.
This “Ultimate Authority Guide” is not another generic overview. It is designed specifically for Clinicians, Gynecologists, and Clinic Owners who are tired of referring patients away. We are going to move beyond basic patient education. We will take a deep dive into the pathophysiology of Male Infertility Causes, align these realities with the nuanced updates in the WHO 2021 (6th Edition) manuals, and outline exactly how partnering with Subhag.in for help with ART clinic registration and specialized Andrologist training can transform your practice from a simple consulting room into a Tier-1 fertility destination.
1. The Epidemiology of Male Infertility in India (2024 Data)
We need to talk about the “Indian Male.” He is facing a quiet fertility crisis. If you look at the studies published by the Indian Council of Medical Research (ICMR) or track the independent longitudinal data, the trend line is undeniable: sperm quality parameters have been in freefall over the last two decades. Understanding the sheer scale of this decline is vital for any clinician planning to start your IUI clinic.
The Statistical Shift
- Prevalence Rates: In my experience, the textbooks are lagging behind reality. Current estimates suggest that nearly 10-15% of Indian couples face infertility. But here is the kicker: the male factor is solely responsible in 20-30% of these cases and is a contributing co-factor in another 30%. That means in half the couples you see, the male needs medical attention.
- Urban vs. Rural: Ten years ago, we thought this was just an urban phenomenon—the result of corporate stress and laptop heat. We were wrong. Data now suggests rapidly rising rates of Male Infertility Causes in Tier 2 and Tier 3 cities. In agrarian belts, I suspect pesticide exposure is playing a massive, under-reported role, alongside the lifestyle shifts sweeping the nation.
- The “Referral Leakage”: Let’s look at your numbers. If you run a standard gynecology OPD seeing 50 infertility patients a month, statistically, 25 of those couples have a male factor issue. If your clinic cannot diagnose or treat these men, you are effectively turning away 50% of your potential business. You aren’t just losing a sperm wash fee; you are losing the IUI cycle, the medications, and the patient loyalty.
For the astute clinician, this data presents a clear mandate: Integration of Andrology services is not optional; it is essential for survival and growth in a hyper-competitive fertility market. By identifying specific Male Infertility Causes early, you retain the couple. You perform the IUI cycles in-house. And most importantly, you improve your success rates, which is the best marketing you can ever buy.
Reference: PubMed: Declining Sperm Count trends in the Indian Subcontinent
2. Pathophysiology: Classifying Male Infertility Causes
To treat effectively, one must diagnose accurately. It sounds simple, but as a gynecologist expanding into IUI, you have to move beyond the simple “Low Sperm Count” label. That label is a symptom, not a diagnosis. We must categorize Male Infertility Causes based on the physiological breakdown. This classification is what tells me whether a patient is a candidate for simple medical management and IUI, or if he needs an immediate referral for ICSI to avoid wasting time and money.
Pre-Testicular Causes (Endocrine & Hypothalamic)
These causes stem from the disruption of the HPA (Hypothalamic-Pituitary-Gonadal) axis. While they are rarer—popping up in maybe 1-2% of cases—I love finding them. Why? Because they are often the most treatable.
- Hypogonadotropic Hypogonadism: This is essentially a failure of the pituitary to secrete FSH and LH. Patients present with low testosterone and azoospermia or severe oligospermia. I’ve seen men with zero sperm count respond brilliantly to Gonadotropin therapy. These patients can often become excellent candidates for IUI after induction, transforming a “hopeless” case into a pregnancy.
- Hyperprolactinemia: Elevated prolactin levels inhibit GnRH pulsatility. It’s an easy fix if caught.
- Thyroid Disorders: Both hyper- and hypothyroidism can impair spermatogenesis. Never skip the TSH.
Testicular Causes (Primary Failure)
These are intrinsic defects within the testes affecting spermatogenesis. In the daily grind of the clinic, this is the most common category of Male Infertility Causes you will encounter.
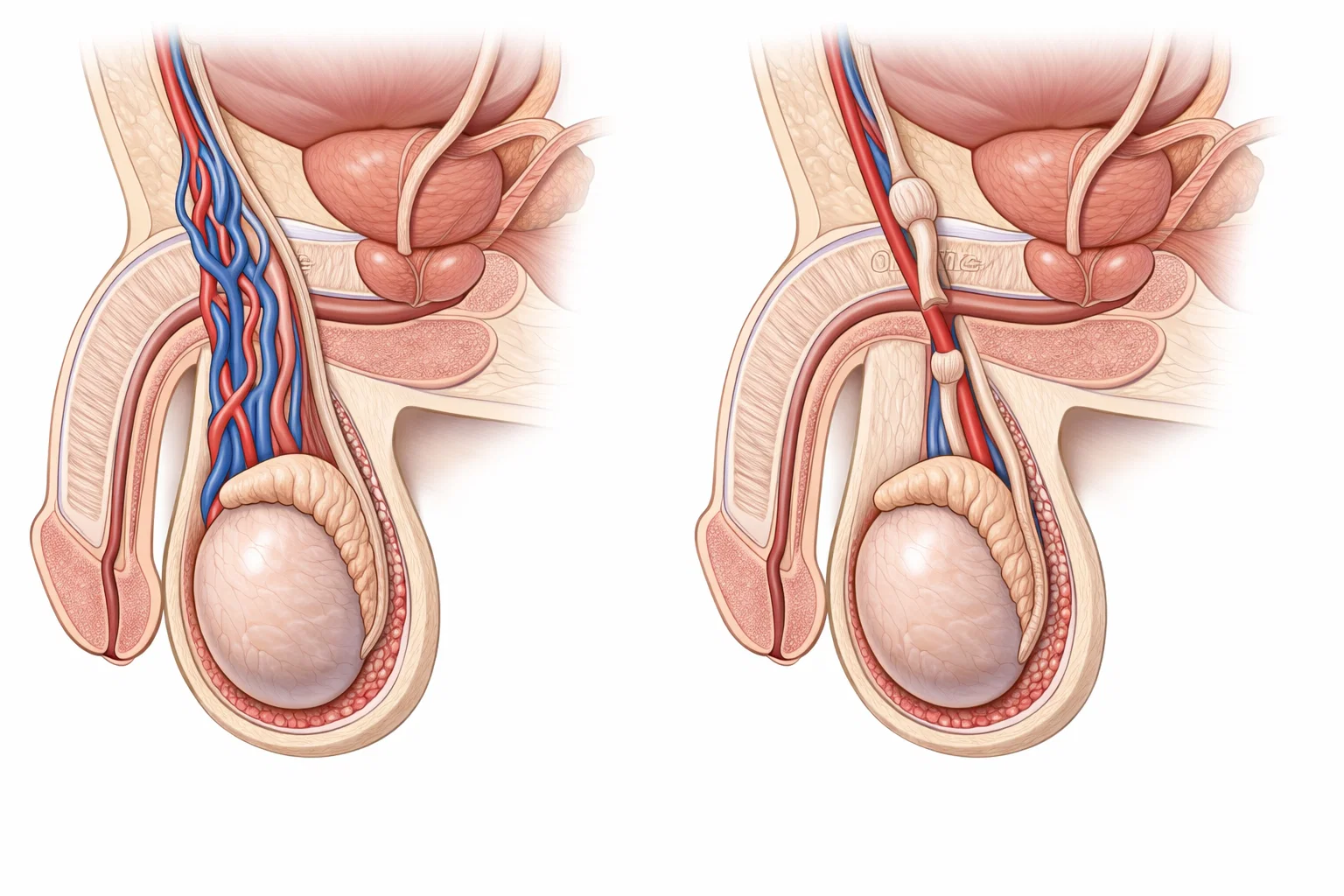
- Varicocele: The dilation of the pampiniform plexus is controversial, but significant. It causes hyperthermia and oxidative stress, leading to DNA damage. Here is my rule of thumb: Grade 3 varicoceles might need surgery, but for Grade 1 and 2 with borderline counts, I often manage them effectively with antioxidants and IUI.
- Cryptorchidism: Always ask about childhood surgeries. A history of undescended testes is a major red flag for primary testicular failure.
- Genetic Factors: We see Klinefelter Syndrome (47, XXY) and Y-chromosome microdeletions more often than you’d think.
- Infections: A history of Mumps orchitis can lead to irreversible testicular atrophy. It’s a tragic, silent destroyer of fertility.
Post-Testicular Causes (Obstructive & Functional)
In these scenarios, the factory is working, but the delivery truck is broken. Sperm production is normal, but transport is blocked or functional delivery is impaired.
- CBAVD (Congenital Bilateral Absence of the Vas Deferens): If you see low volume and acidic pH, check for the vas. It’s strongly associated with Cystic Fibrosis mutations.
- Ejaculatory Duct Obstruction (EDO): Often caused by cysts or chronic inflammation.
- Retrograde Ejaculation: Common in diabetic males or post-bladder neck surgery.
- Coital Issues: Erectile dysfunction or premature ejaculation. These are sensitive topics, but they need to be addressed.
Clinical Note: Post-testicular causes like retrograde ejaculation or mild obstructions are often bypassed effectively using sperm retrieval techniques and IUI, provided the clinic has the right Embryologist training protocols in place. It’s about having the skills to recover what is there.
3. Comprehensive Etiology: What Every Fertility Specialist Must Screen For
When taking a history for a couple, the investigation of Male Infertility Causes must be as rigorous as the female workup. Too often, the male history is just “do you smoke or drink?” We need to go deeper. Below is the detailed etiology checklist I use in my practice.
Genetic Factors and Chromosomal Abnormalities
Genetic screening is mandatory for men with severe oligospermia (< 5 million/ml). I cannot stress this enough: failing to identify these can lead to vertical transmission of defects to the offspring.
- Karyotyping: Essential to rule out translocations or aneuploidy. You don’t want to be the doctor who missed a translocation that caused recurrent miscarriages.
- Y-Chromosome Microdeletions (AZF): Deletions in the AZFa, AZFb, or AZFc regions dictate the prognosis. For instance, AZFc deletions may still allow for sperm retrieval, whereas AZFa usually implies Sertoli Cell Only syndrome. Knowing this saves the patient from unnecessary surgeries.
Lifestyle and Environmental Impact (The Modern Plague)
This is where patient counseling plays a massive role. The modern Indian lifestyle is hostile to sperm.
- Oxidative Stress (ROS): The sperm membrane is rich in polyunsaturated fatty acids, making it highly susceptible to Reactive Oxygen Species. High ROS levels are a primary cause of idiopathic infertility and DNA fragmentation.
- Obesity: Adipose tissue is not inert; it’s an endocrine organ. It increases aromatase activity, converting testosterone to estradiol, suppressing spermatogenesis. Tell your patients: “Weight loss is a fertility treatment.”
- Smoking & Alcohol: There is a direct correlation with reduced motility (asthenospermia) and morphology defects (teratospermia).
- Occupational Hazards: I ask every patient what they do for a living. Long-haul truck drivers (heat), software engineers (sedentary/laptop heat), and factory workers (chemical exposure) are at significantly higher risk.
Iatrogenic and Systemic Causes
Review the patient’s medication list meticulously.
Testosterone Replacement Therapy (TRT): This is a growing cause of iatrogenic azoospermia. Many men take testosterone supplements for “gym performance” or libido, unknowingly shutting down their endogenous sperm production via negative feedback. I’ve had to wean countless men off gym supplements to restore their counts.
Chemotherapy/Radiation: History of malignancy requires banking sperm, but if not done, assessment of recovery is crucial.
4. Diagnostic Protocols: Setting Up Your Andrology Lab
You cannot effectively treat what you cannot see. To accurately identify Male Infertility Causes, relying on external labs often results in delayed or standardized reports that lack clinical nuance. I always advise my clients: Setting up an in-house Andrology lab is the first step toward clinic autonomy.
The WHO 2021 Manual (6th Edition) Standards
Subhag emphasizes strict adherence to the latest WHO guidelines. The 6th edition has shifted reference limits slightly, and frankly, if your lab technicians are not aware of these changes, you are misdiagnosing patients.
- Semen Volume: Lower limit 1.4 ml.
- Sperm Concentration: 16 million/ml (previously 15).
- Total Motility: 42% (previously 40%).
- Morphology: 4% (strict Tygerberg criteria). This is the hardest one to get right without training.
If your current setup or referral lab is still using 1999 or 2010 standards, you are working with a broken compass.
Advanced Sperm Function Tests
A standard semen analysis (SA) is just a headcount. It misses functional defects. A modern IUI clinic must offer more depth:
- Sperm DNA Fragmentation Index (DFI): I consider this a vital metric. High DFI (>30%) is often the hidden cause of “Unexplained Infertility” and Recurrent Pregnancy Loss (RPL). It is a critical metric for deciding between IUI and IVF. If DFI is 40%, IUI is likely a waste of time.
- HBA Assay (Hyaluronan Binding Assay): Tests sperm maturity and ability to bind to the egg.
- ASA (Anti-Sperm Antibodies): Crucial for ruling out immunological infertility, where the body attacks its own gametes.
- LeucoScreen: To differentiate between round cells (immature sperm) and leukocytes (infection). Treating a “high round cell count” with antibiotics when it’s actually immature sperm is bad medicine.
Strategic Insight: Implementing these tests requires skilled personnel. You can’t just buy the kit; you need the expertise. Subhag provides comprehensive Embryologist training to ensure your staff can perform and interpret these advanced diagnostics accurately, keeping the revenue within your clinic.

5. From Diagnosis to Treatment: The IUI Clinic Model
Once you have identified the specific Male Infertility Causes, the next step is formulating a treatment plan. This is where the clinical science meets the business of your practice.
Medical Management
Before we jump to ART, optimizing the male gamete can drastically improve IUI success rates.
Antioxidants: I typically start men on CoQ10, L-Carnitine, and Zinc supplementation for 3 months. It’s not magic, but it helps.
Hormonal Stimulation: The use of Clomiphene Citrate or Tamoxifen in men with low-normal testosterone to boost FSH/LH drive is an old trick, but it often works to bump the count just enough for IUI.
Sperm Preparation Techniques for IUI
The days of the “One size fits all” sperm wash are over. Your lab protocol should vary based on the diagnosis:
- Double Density Gradient: The gold standard for removing debris, leukocytes, and immature sperm. It is ideal for teratospermia or high viscosity samples.
- Swim-Up Method: Best for samples with high motility but low volume, ensuring only the most motile, competent sperm are selected.
- Microfluidics (Emerging): For high DFI cases, this technology sorts sperm without centrifugation stress, preserving DNA integrity.
When to Refer for IVF/ICSI
Ethical practice builds trust. Establishing cut-offs is key. Generally, a Total Motile Sperm Count (TMSC) of < 5 million post-wash is considered the threshold where IUI efficacy drops significantly. In these cases, IVF/ICSI should be recommended. However, for counts between 5-10 million, IUI remains a highly cost-effective first line, and patients appreciate being given that option.
6. ART Registration and Legal Compliance (The ART Act 2021)
We have to address the elephant in the room. Treating male infertility in India is now a highly regulated activity. The Assisted Reproductive Technology (Regulation) Act, 2021, mandates strict compliance. The days of simply “doing IUI” in a side room are gone.
- Level 1 vs. Level 2 Clinics:Level 1 (IUI Clinics): These are permitted to perform Intrauterine Insemination. They require specific infrastructure, a qualified gynecologist, and designated lab areas.Level 2 (IVF Clinics): These are permitted to perform oocyte retrieval and embryo transfer.
- Documentation: You must maintain rigorous records of the Male Infertility Causes diagnosed, consent forms for husband’s sperm (or donor sperm) usage, and chain of custody for samples. The paperwork is tedious, but necessary.
- The Subhag Advantage: The paperwork for registration can be overwhelming. I’ve seen doctors give up on their IUI plans just because of the forms. Subhag assists Gynecologists with end-to-end help with ART clinic registration, ensuring your floor plan, equipment list, and staff qualifications meet the National Registry requirements perfectly.
Reference: ICMR Guidelines for ART Clinics in India
7. The Economics of Treating Male Infertility
Why should a Gynecologist invest in an Andrology setup? Apart from better patient care, the Return on Investment (ROI) is compelling.
Cost of Setup in India
Setting up a Level 1 IUI lab is not capital intensive compared to a full IVF setup. You don’t need micromanipulators yet. Essential equipment includes a Laminar Air Flow (LAF), Centrifuge, Incubator, and a high-grade Microscope. With Subhag’s vendor network, this cost is optimized without compromising on quality.
Revenue Modeling
Consider the revenue leakage of referring out. Every time you send a patient away, you lose:
Semen Analysis: Avg ₹500 – ₹1000.
Sperm DNA Fragmentation: Avg ₹4000 – ₹6000.
IUI Cycle (Stimulation + Wash + Insemination): Avg ₹8000 – ₹15,000 per cycle.
For a clinic managing just 20 IUI cycles a month, the revenue from treating Male Infertility Causes in-house can add ₹2 Lakhs to ₹3 Lakhs monthly to the bottom line. You typically recover the setup cost in less than 6 months.
8. The Critical Role of Professional Training
I have visited clinics with top-tier German equipment that yields zero results because of incompetent handling. The biggest bottleneck for new IUI clinics is not the machinery; it is the lack of trained staff.
- Gynecologist Training: You need to master the art of ovarian stimulation protocols specifically tailored for male factor cases. For example, mild stimulation to target 2-3 follicles increases probability, counteracting the male factor. Subhag offers specialized Gynecologist training modules to refine these protocols.
- Andrologist/Embryologist Training: Your lab technician or junior doctor needs hands-on skills in semen processing. A bad wash can ruin a good sample. Our Andrology training covers WHO manual compliance, QC/QA in the lab, and equipment maintenance.
Subhag.in bridges this gap by offering short-term, intensive, hands-on Fertility training programs designed for busy clinicians who need practical skills, not just theory.

Frequently Asked Questions (FAQs) for Clinicians
Clinical Diagnostics
Q1: What is the new lower reference limit for sperm concentration according to WHO 2021?
A: The 6th Edition sets the lower reference limit at 16 million/ml (up from 15 million/ml in the 5th Edition). It’s a small shift, but clinically significant for borderline cases.
Q2: How does high DFI affect IUI success rates?
A: High DNA Fragmentation Index (>30%) correlates with significantly lower pregnancy rates and a higher risk of early miscarriage in IUI. In such cases, I usually recommend antioxidant therapy or moving straight to IVF/ICSI.
Q3: Is scrotal ultrasound mandatory for all male infertility cases?
A: Not always, but I recommend it if varicocele, testicular mass, or obstruction is suspected clinically, or if the physical exam is difficult due to anatomy (e.g., tight scrotum).
Q4: How do I differentiate between obstructive and non-obstructive azoospermia?
A: Look at the FSH. Normal FSH with normal testicular volume usually suggests obstruction. High FSH with small testes suggests failure. The confirmation, of course, is biopsy.
Q5: Can I treat retrograde ejaculation with IUI?
A: Yes, and it’s very satisfying when it works. The protocol involves urine alkalinization followed by sperm retrieval from the post-ejaculatory urine, washing, and performing IUI.
Treatment Protocols
Q6: What is the cut-off TMS (Total Motile Sperm) count for IUI?
A: Generally, a post-wash count of >5-10 million yields the best results. Counts between 1-5 million have very low success rates (~2-3%), so manage expectations.
Q7: What is the role of antioxidants in idiopathic male infertility?
A: Cochrane reviews suggest improvement in live birth rates. I typically prescribe a combination of L-Carnitine, CoQ10, Zinc, and Selenium for a minimum of 3-6 months.
Q8: How do I manage patients with anti-sperm antibodies (ASA)?
A: IUI is actually an effective first-line treatment here, as the sperm washing process—especially chymotrypsin digestion—reduces the antibody load significantly.
Q9: Is genetic testing mandatory before IUI?
A: Not for every patient. However, it is mandatory for severe oligospermia (< 5 million/ml) to rule out chromosomal defects like Klinefelter or Y-deletions before proceeding.
Q10: What is the best sperm preparation method for viscous semen?
A: Mechanical disruption (gentle pipetting) or limited enzymatic digestion followed by Density Gradient Centrifugation is my preferred method.
Business & Regulatory
Q11: Do I need a full-time Embryologist for an IUI clinic?
A: For Level 1 clinics, a full-time senior embryologist is not mandatory. You can train your existing lab staff via Andrologist training or hire a visiting embryologist.
Q12: What is the minimum lab space required for ART registration?
A: The National Registry mandates specific square footage (often separate areas for collection, processing, and insemination). Subhag assists in compliant layout planning to ensure you don’t fail inspection.
Q13: How long does ART registration take in India?
A: It varies by state, but typically expect 3-6 months depending on the authority’s inspection schedule and your document readiness.
Q14: Can a Gynecologist perform Semen Analysis?
A: Yes, provided they have documented training. Our Gynecologist training covers this module thoroughly.
Q15: What is the average ROI period for an IUI lab setup?
A: With a modest patient flow of 10-15 cycles/month, break-even on equipment cost is often achieved within 6-9 months.
Subhag Partnership
Q16: Does Subhag help with equipment procurement?
A: Yes, we provide end-to-end setup guidance, helping you choose the right centrifuges, microscopes, and consumables.
Q17: Is your training recognized for ART registration?
A: Our training aligns with professional standards required for competency demonstration during inspections.
Q18: How does Subhag assist with patient marketing?
A: We provide branding support and digital presence strategies to help you attract patients specifically seeking solutions for Male Infertility Causes.
Q19: Can you help scale from IUI to IVF later?
A: Absolutely. Our infrastructure planning accounts for future scalability, ensuring your IUI lab can be upgraded to an IVF lab seamlessly when you are ready.
Q20: What support do you offer for male infertility cases that fail IUI?
A: We offer a network of advanced senior embryologists for consultation on difficult cases and advice on further referrals.
Conclusion: Partnering for Clinical Excellence
Understanding Male Infertility Causes is the first step in a much larger journey. For the Indian Gynecologist, the transition from a purely consulting practice to a procedure-based fertility clinic is the logical path to professional and financial growth. However, this path requires more than just clinical intent; it requires infrastructure, compliance, and specialized skills.
Don’t let a lack of infrastructure or training hold your practice back or force you to refer away valuable patients. Join the growing network of successful Gynecologists who have partnered with Subhag.in for their IUI clinic setup, help with ART clinic registration, and professional training.
Ready to launch your IUI clinic and treat male infertility effectively? Contact Subhag today for a free consultation on lab setup and training. Let’s build your clinic together.
Additional Resources:
ESHRE Guidelines on Male Infertility
WHO Laboratory Manual for the Examination and Processing of Human Semen (6th Ed)


